
Next advancement in robotic surgery seen in Las Vegas
























“Don’t forget to deploy for docking,” the da Vinci Xi says, sounding as polite as any machine can. “Now, install the endoscope.”
Minutes later, Dr. Shawn Tsuda’s voice echoes through the University Medical Center operating room over the same sound system.
“Go in deeper if you can,” Tsuda tells a resident assisting with the procedure. “Right there!”
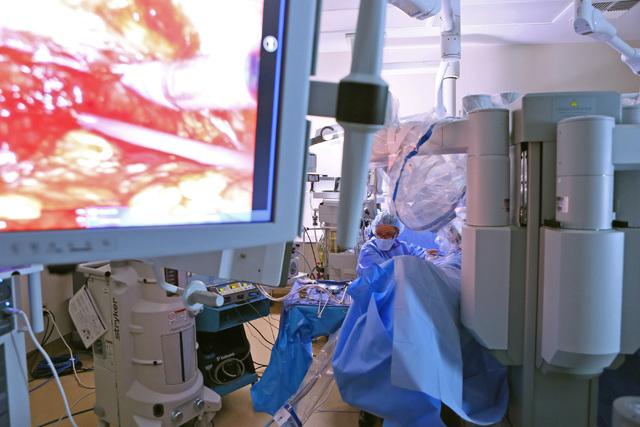
Tsuda and the Xi, joined as one, were about to begin a hernia repair and gallbladder removal, two of the most common procedures performed in the abdomen. The next generation of robotic surgical system makes Tsuda’s job as minimally invasive as the procedures can be, delivering smaller incisions, less blood loss, fewer complications and shorter recovery periods.
The advantages of robotic surgery are becoming available to more patients in Southern Nevada as hospitals acquire more of the systems and more surgeons become adept at their use. The spread and prevalence of robotic surgery is limited only by finite resources and the learning curve of the men and women at the controls.
In addition to UMC, Sunrise, MountainView and Valley hospitals have the Xi, which offers greater range of motion and reach than its predecessor, the da Vinci Si. Both systems are distributed by Intuitive Surgical, based in Northern California, which has sold 212 Xi systems nationwide. The devices sell for $1 million to $1.5 million depending on how many features are included in the package, company spokesman Justin Higgs says.
Doctor and patient demand and community need motivate hospital officials to buy the da Vinci Xi, not just because the device is minimally invasive, but also because the system can be employed for the most complex of cases. For such an expenditure to be a wise investment, the system must appeal to doctors already practicing at the hospital and others who would bring cases there after the acquisition.
It’s no coincidence that the four Xi systems in Southern Nevada are at the three teaching hospitals and MountainView, which plans to begin a general surgery residency program next year.
“An increasing number of physicians are adopting that technology,” UMC CEO Mason VanHouweling says. “We felt it was important that new doctors had the ability to train on this equipment at UMC.”
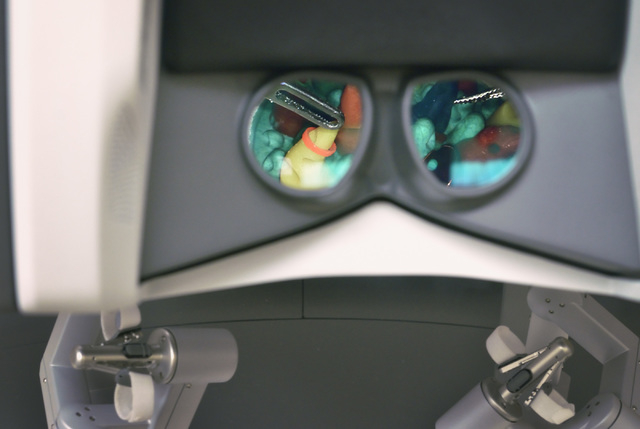
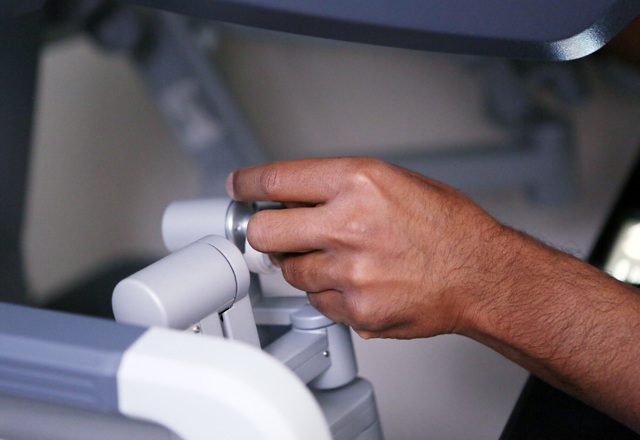
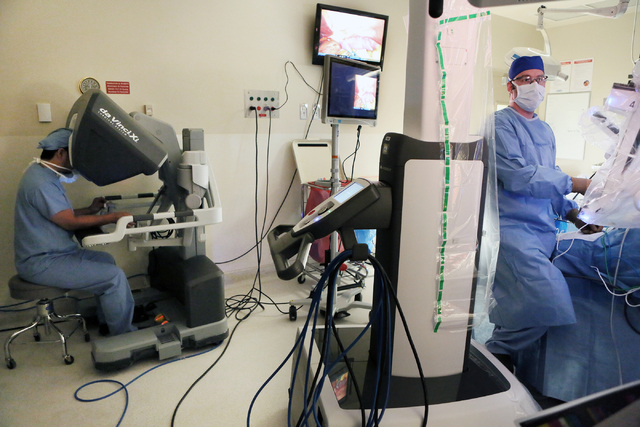
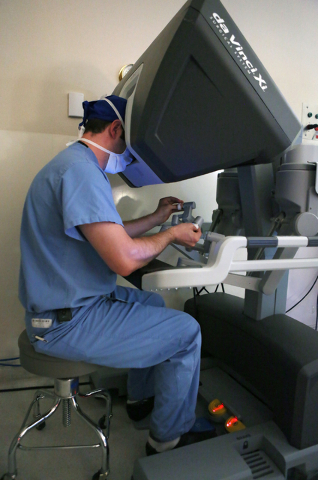
In robotic surgery, procedures are completed with small tools at the end of ports attached to a robotic arm. The ports are inserted through the keyhole incisions in the abdominal wall. The surgeon, sitting at a console about 6 feet away, operates the robotic arms via computer from hand controls similar to a video game.
The process should be called computer-assisted surgery because the doctor always is in control of the robot.
TREMENDOUS ADVANCEMENTS SEEN
The development of laparoscopic techniques in the 1990s helped doctors achieve tremendous advancements in abdominal surgery in terms of minimizing patient recovery times and post-operative complications.
Laparoscopy relies on small incisions for inserting tubes with cameras and tools for examinations and procedures. Laparoscopy can help diagnose conditions or perform operations in a less invasive manner than regular open abdominal surgery.
The robotic systems have improved those outcomes a step further, but the improvement over laparoscopy is not as pronounced as the advances made in the ’90s. Traditional open surgeries require big incisions, leading to more blood loss and pain, and longer healing times than if a surgeon can operate through a keyhole. Laparoscopy minimizes the incisions, but the tools still are in the hands of the surgeons, prone inefficient movements. Tsuda calls laparoscopy operating with chopsticks.
The incrementally better outcomes in robotics over laparoscopy are believed to be linked to the steadiness the robotic arms provide, limiting the stress to the muscles and tissues of the abdominal wall. In addition, the robotic systems provide better visualization, giving the doctor more magnification and a three-dimensional view, and enhanced control over the surgical tools.
The surgeon can move the hand controls farther than the tools move inside the body, a technique known as motion scaling.
“In an open procedure, if I move an instrument 2 inches, my hand has to move 2 inches,” says Dr. Victor Grigoryev-Grigg, a Las Vegas urologic surgeon. “In robotic surgery, my hand can move a full foot, but the actual instrument moves only inches.”
That eliminates hand tremors, and lets the surgeon target tissues with much greater ease. Once proficient on the robotic system, the surgeon gains a finesse that surpasses human capabilities.
PROGRESS FROM EARLIER SYSTEMS
Grigoryev-Grigg remembers the earliest robotic surgical systems, the Aesop and Zeus, which provided little more than extra hands for surgeons who needed more than two probes employed at a time.
“They were more like an assistant to the surgeon,” he says. “The robot would move the instrument by command, but there was no three-dimensional view and no scaling.”
The da Vinci systems refined the process further, facilitating movements that are more intuitive. Surgeons say the change from the da Vinci Si to the da Vinci Xi provides another “incremental advancement” because the Xi can move in ways the Si cannot.
“Xi helps when you have to do surgery in different parts of the abdomen during the same procedure if you have to move around quite a bit,” Grigoryev-Grigg says. “The way that the arms are positioned and the way that it’s designed ergonomically, you can move from the pelvic area to the left part of the abdomen to the upper abdomen fairly easily, which you cannot always do with the Si.”
That flexibility minimizes risks to the patient.
“That has an effect on many safety issues in the operating room,” Tsuda says. “It can affect anesthesia. It can affect sterility. It can affect timing.”
Many of the surgeons performing robotic procedures in Southern Nevada learned the techniques after completing residencies and fellowships and starting their practices. Not all physicians can afford to put their practices on hold to go through special training in robotics.
Dr. Jayram Krishnan is one doctor who did. Krishnan, who recently performed the first robotically rebuilt urinary bladder in Las Vegas at Sunrise, worked with three mentors on some 200 cases over the course of a year at the Cleveland Clinic on a fellowship to become proficient in robotic surgery techniques.
Today’s residents are learning during their training. Residents first observe attending physicians and can gain additional expertise practicing on cadavers. The da Vinci systems also have computer simulations to give surgeons-in-training more experience.
“You can sit and simulate parts of certain procedures so you can get very, very familiar with the techniques without actually operating on a patient,” says Dr. Ovunc Bardakcioglu, the University of Nevada School of Medicine’s director of robotic surgery. “In the past, that didn’t exist. When I learned open surgery, there were no simulators. It was learning by doing.”
LAS VEGAS ‘WAY AHEAD’ OF OTHER CITIES
Those simulators also provide feedback, showing whether the resident has grasped the technique.
At the Las Vegas Institute for Robotic Surgery at MountainView, Dr. Arnold Chung, cardiovascular and thoracic surgeon, soon will be training doctors from across the nation in the latest technology.
Tsuda says the learning curve for robotic surgery is much less than when a surgeon develops laparoscopic techniques.
“When you’re working with a lap, you can tell right away who’s experienced and who’s not,” he says.
Robotic surgical procedures will continue to expand as data show how outcomes improve. Sometimes that data can take decades to acquire, and Southern Nevada medical professionals are trying to contribute to that base of knowledge. Bardakcioglu and Tsuda are among a group of doctors planning to research whether residents trained on simulators learn faster than those who do not.
The doctors have applied for a grant to research the issue, but Bardakcioglu likes their chances of securing the funding.
“In terms of robotics, Las Vegas is way ahead of a lot of other cities nationally,” he says.
Contact Steven Moore at smoore@reviewjournal.com or 702-380-4563.



















